THE PROXIMAL GOLD FOIL FILLING
INVOLVING THE INCISAL ANGLE
A. B. BUTTER, D.D.S., R. O. GREEN, D.D.S., and W. J. SIMON,
D.D.S.,
Minneapolis,
Minn.
From the University
of Minnesota, School of Dentistry,
Department of Operative Dentistry.
Jour. A.D.A., Vol. 30, December t, 1943
TO those interested in gold foil, cavities in the proximal
surfaces of the incisor teeth which involve the incisal angle present
interesting possibilities. The chief objection to this type of filling from
the patient's point of view is the display of gold. While it is conceded that
the operation involving the incisal angle is necessarily extensive, it is
possible, by judicious cutting, to develop the outline form so that the
filling, when finished, will be far less conspicuous.
CAVITY PREPARATION
Contrary to the teachings of some operators, the proximal
labial margin should be a straight line from the incisal edge to a point
beneath the free margin of the gingiva parallel to the long axis of the tooth,
and as close to the embrasure as is consistent with the principles of extension
to areas of relative immunity. (Fig. 1, A.) If this cut is made otherwise, as,
for instance, parallel with the proximal surface of the tooth, there will
develop at the incisal angle an unsupported area of enamel which will prove a
menace in condensation, and the finished result will be out of harmony with the
tooth.
The amount of tooth structure cut from the incisal edge will
depend on the type of tooth and the stresses placed upon the incisal angle.
Ordinarily, the incisal cut is carried two-thirds of the way across the incisal
edge (Fig. 1, B), thus securing a greater leverage for the filling, which will
be anchored by an incisal retention form. A cut which is not past the middle
lobe of the tooth places the retention form in a position which may embarrass
the pulp.
By crossing the incisal edge labio-lingually, at an angle of
450, additional resistance to masticatory stresses from the lingual
aspect is obtained. (Fig. 1, C ) This cutting can be done with a carborundum
stone. The proximal lingual wall can be cut down to a point below the free
margin of the gingiva with a straight chisel. (Fig. 1, D.) The
proximo-linguo-incisal angle is well rounded off, as indicated by the dotted
line in Figure 1, D.
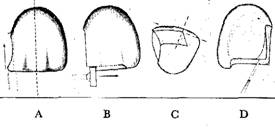
Fig. 1. A, proximo-labial margin parallel to long
axis of tooth. B, incisal cut carried approximately two-thirds of way across
incisal edge. C, crossing incisal edge at an angle of 450 to obtain
additional resistance to masticatory stresses from the lingual aspect. D,
proximo-linguo-incisal angle well rounded off.
In cutting across the incisal edge, the stone is held in
such a manner that the lingual enamel plate is reduced more than the labial
plate. (Fig. 2, A.) Because of the stresses upon the tooth, the shape of the
tooth and the thickness of the labial and lingual enamel plates, it is not
possible to state dogmatically how much of the lingual plate should he removed.
Generally speaking, it is at least twice as much as the enamel removed front
the labial plate. One of the methods of reducing the lingual plates is to
undermine the lingual enamel with a small single cut fissure bur. (Fig. 2, B.)
With the chisel, as illustrated in Figure 2, C, the enamel is cleaved away, to
effect the "incisal step." Some operators reduce the lingual enamel
plate with small inverted cone stones, as shown in Figure 2, D. The
"incisal step" is to be finished smoothly with special burs, stones,
chisels and cuttle disks when accessible.
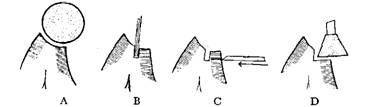
Fig. 2.—A, initial reduction of lingual enamel
plate. B, undermining of lingual enamel plate. C, cleaving away of undermined
enamel. D, finishing "incisal step."
The proximal portion of the cavity should he extended far
enough to free contact with the adjacent tooth. The gingival seat should either
be flat (Fig. 3, A) or should follow somewhat the curvature of the cervical
line. An inverted cone bur is useful here provided care is taken that it is
not brought too far labially or lingually. Primarily, the gingival seat must be
so constructed that it presents a flat surface at least at right angles to the
line of incisal stress.
A B
Fig. 3.—A, gingival seat. This should be flat. B,
gingivo-axial line slightly acute, as is preferable.
Substantial retentive resistance form, which is necessary
for this filling, is secured by means of two point angles at the gingival
portion and an incisal retention form at the far end of the incisal step. The
gingival point angles are started with a small single-cut fissure bur. (Fig. 4,
A.) The direction of the gingival retention forms are such that they all times
to be in dentin between the bisect the point angles. The bur is at pulp and the
dentino-enamel junction. The depth to which this bur is projected is a matter
of judgment, depending on the size of the cavity and the stresses to be exerted
on the filling.
The bur is also drawn up the labio-axial and linguo-axial
line angles approximately a third of their length. These line angles are now
emphasized and accentuated by the use of small monangle hoes. (Fig. 4, B.)
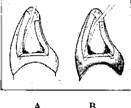
Fig. 4.—A, gingival point angles started with small
single cut fissure bur. B, line angles accentuated by means of rnonangle hoes
Probably not more than a third of the linguo-axial line
angle can be used for retentive resistance forms, but that portion which is
available must be utilized to the fullest extent.
The labio-axial line angle, while it may be generally
obtuse, should be prepared in a definite manner. For example, Figure 5, A is a transverse
section at the gingival seat, showing a retentive labio-axial and linguo-axial
line angle which is definitely an acute angle. At the junction of the gingival
third and the middle third, the labio-axial and linguo-axial line angles
approximate a right angle. (Fig. 5, B.) In the middle third (Fig. 5, C), both
line angles are obtuse and, in the incisal third (Fig. 5, D), the line angle
fades out, leaving as much dentin as possible to support the enamel plates.
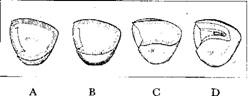
Fig. 5.—A, labio-axial and linguo-axial line
angles, which are definitely acute angles. B, line angles approximating right angle.
C, line angles obtuse. D, line angles fading out.
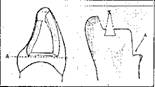
The incisal step presents a flat ledge on the lingual
aspect, which is all-important in the resistance of the filling to masticatory
stress. The labial wall of this step is cut parallel with the long axis of the
tooth, a triangular portion of dentin remaining to support the labial plate.
Retention is further secured by cutting a rectangular form at the far end of
the incisal step. Usually, this retention is made with a small single cut
fissure bur slightly undercutting the mesial and distal walls as indicated by
the letter X in Figure 3, B. This incisal retention form should he cut as large
as is consistent with the area involved. Generally, it is made too small for
the purpose for which it is intended. The incisal retention form should he
directed gingivally parallel to the labio-incisal plate of enamel, keeping well
within dentin and away from the lingual enamel plate. (Fig. 6.)
The cavosurface angles of the cavity should he planed and
disked when accessible. The gingival ,cavosurface is beveled with a monangle
hoe. Any other part of the cavity in which there is any doubt regarding
unsupported enamel is also beveled. There should never be any angles as such in
the outline form to disturb the harmony of tooth outline form.

Fig. 6. Incisal retention form directed gingivally
parallel to labio-incisal plate of enamel.
The completed
cavity is presented in Figure 7, from various aspects in recapitulation of
some of the key points of the cavity preparation.
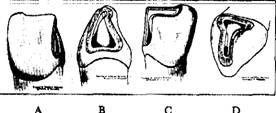
Fig. 7.—A,
proximolabial aspect of finished cavity, showing proximolabial margin
parallel to long axis of tooth and incisal cut carried approximately two-thirds
of way across incisal edge. B, proximal aspect, illustrating "incisal
step" and accentuation of labia-axial and linguo-axial angles from
retention forms. C, proximolingual aspect; The proximolingual incisal angle is
well rounded off. D, proximo-incisal aspect of finished cavity, showing incisal
retention form and acute gingivo-axial line angle.
CONDENSING AND
FINISHING
To condense-gold foil properly, the force should be in as
nearly a direct line as possible to the long axis of the tooth, so that the
peridental membrane may resist the pressure demanded in filling. The plugger
points should be cleansed frequently and the serrations freed of gold
adhesions. The amount of force applied in condensing gold foil will be governed
not only by the surface area of the plugger points, but also by the tolerance
of the patient. In the cavity preparation herein described, the approach is
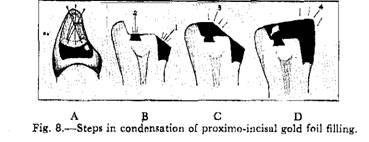
toward the incisal aspect. Regardless of the type of plugger point, the gold
foil is being wedged continually between the labio-axial wall and the
linguo-axial wall. (Fig. 8, A.) The foil should be stepped continually from the
center of the mass of previously condensed gold foil toward one of the walls.
The gold foil is started in both of the gingival point
angles, building up the axial wall at an angle of 450 (Fig. 8, B), care
being taken to carry the foil out to the full contour as we proceed. If this is
not done at this time, it will be difficult to go back and fill in the
deficiencies later. When the filling has reached the "incisal step,"
the foil is started in the incisal retention form and condensed across the
incisal to meet the proximal portion. (Fig. 8, C.) The incisal portion and the
proximal portion are welded together and, by maintaining condensation in line
with the long axis of the tooth, the filling is built up to full contour. (Fig.
8, D.)
After burnishing the gold over the margins, the surplus is
trimmed off with knives, chisels, files, stones, disks and strips and the
filling brought to shape and contour. In the final finishing of the
proximo-incisal gold foil, it is essention not only to recover the original
esthetic outline created, but to restore the harmonious proportions in the varying
curves and angles of the tooth.
VARIATIONS
There are other methods of treating cavities in the proximal
surfaces of incisors in which the incisal angle has become involved. Every
operator wishes to display as little gold as is commensurate with the stresses
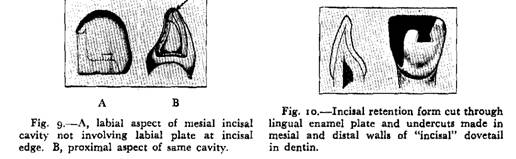
placed upon the filling. In cases of marked overjet, it is possible to prepare
cavities which do not display any gold in the incisal edge. A cavity of this
type is illustrated in Figure 9, A and B.
In delicately shaped incisors with a short labio-lingual
diameter, the operator will experience difficulty in finding sufficient dentin
between the labial and lingual plates of enamel for the incisal retention form.
In this type of case, the incisal retention form is cut through the lingual
enamel plate and undercuts are made in the mesial and distal wall of the incisal
dovetail in dentin for retention. (Fig. 10)
In incisors with a short labio-lingual diameter, the incisal
retention form is cut through the lingual enamel plate and undercuts are made
in the mesial and distal walls of the "incisal" dovetail in dentin
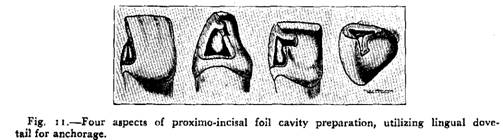
for retention. (Fig.10) Another method of treating a proximal cavity which
involves the incisal angle is to prepare the proximal portion in the orthodox
manner, but, in place of cutting down the incisal edge for resistance, prepare
a lingual dovetail for additional anchorage and resistance. (Fig. 11 ) This
cavity can be prepared only in teeth which have a marked labio-version. In
teeth with a linguo-version, it is definitely contraindicated. This lingual
dovetail should be placed as close to the incisal edge as is consistent with
the bulk of the tooth structure to prevent undue leverage from damaging the
incisal angle.
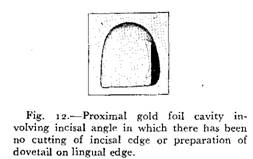
In short teeth that are thick labio-lingually, it is
occasionally possible to prepare a cavity involving the incisal angle without
any special treatment other than establishing a bulky incisal retention form.
(Fig. 12.) The involved incisal angle is slightly rounded to protect the
enamel rods on the incisal edge. This preparation can be used only in those
cases in which the lateral excursions of the opposing teeth do not place undue
stress on the filling.
While the preparation illustrated in Figure 12 is considered
in certain cases, it has been observed that gold foil under heavy stress has a
tendency to pull away from the axial wall and to open at the incisal margin.
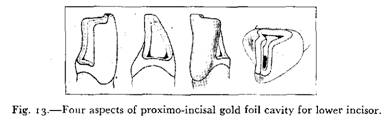
In preparing a proximo-incisal cavity for gold foil in the
lower incisors, a consideration of masticatory stress is important. In cases of
overbite, both normal and abnormal, it will be necessary to remove more of the
labial enamel plate than the lingual enamel plate in lower incisors. (Fig. 13.)
The anatomic form of a lower incisor is of such nature that
frequently the linguo-axial wall need not be extended for the access desirable
in an upper incisor. Likewise, in lower incisors, it is the linguo-axial line
angle that is accentuated in much the same manner as the labio-axial line
angle in upper incisors. In the lower incisors, the incisal retention form is
placed in dentin between the labial enamel plate and the lingual enamel plate.
This requires discretion, since it is very easy to involve a pulp in a lower
incisor.
The cavity illustrated in Figure 13 is considered the normal
cavity. It too is subject to variations depending on the form of the tooth in
question and the relationship of the tooth to the adjacent and opposing teeth.
SUMMARY
In the past, the masters of the gold foil art have shrouded
the proximo-incisal foil cavity preparation with a veil of complexity. In
reality, the proximo-incisal foil cavity is less difficult to prepare than the
strict proximal foil cavity, largely because it is readily accessible. All gold
foil cavity preparation is based upon fundamental principles, which may be
varied in singular cases. The condensing of gold foil into a proximo-incisal
cavity is exacting, requiring skill which is acquired only by perseverance.
Perfectly condensed, properly contoured gold foil fillings in a proximo-incisal
cavity of harmonious proportions have no equal.
This Article was scanned & edited by Dr. John R Sechena
11/2004