OPERATIVE DENTISTRY, 1976, 1, 1, 7-11.
GOLD FOIL IN TODAY'S PRACTICE
Gerald D. Stibbs, B.S., D.M.D
.
Department
of Restorative Dentistry SM-56, University of Washington, School of Dentistry, Seattle, Washington 98195, U.S.A.
Dr. Stibbs is professor of restorative dentistry at the
University of Washington, where formerly he has been chairman of the
Department of Operative Dentistry and chairman of the Department of Fixed
Partial Dentures, director of the dental operatory
and clinical coordinator. He
is a charter member, past president, and past secretary of the American Academy
of Gold Foil Operators, past president of the British Columbia Dental
Association and of the Vancouver (B.C.) Dental Society and instructor of three
gold foil study clubs—the George Ellsperman Gold Foil
Seminar, the Vancouver Ferrier Study Club, and the Walter K. Sproule Study Club. He also has a part-time private
practice.
Renewed interest in prevention and conservative therapy
emphasizes the need for gold foil.
What is the status of the direct golds
in restorative dentistry today? For many years gold foil has been placed on
either the highest or the lowest rung of the ladder in our list of restorative
materials, depending on one's indoctrination, training, or experience with it,
and on whether one is a student, a candidate for a state board examination, or
a member of a foil study club.
Operative dentists may be grouped into three categories in
respect to the use of direct golds. Some, because
their practices are limited to other phases of dental service or because they
harbor a deep-seated aversion to foil, do not use it at all. Others, while
acknowledging the merits of these restorations, use them only occasionally,
due to habit, because of pressures of practice, or because their training in
foil was deficient and they have an anxiety regarding the material. Finally,
there are those who use the direct golds enthusiastically
where indicated.
With space and time limited, it is unlikely that the
unbelievers can be changed, and the active users are as knowledgeable on the
subject as is the author. The most fertile ground is with those who earnestly
want more information and are wondering just how satisfactory the direct golds are today as a restorative medium and how to acquire
a comfortable, effective technique in their use.
Why Gold Foil Is
Important
One reason foil is avoided by many is that it lends itself
admirably to being a testing medium in schools and on State Board examinations,
since in just one operative appointment an examiner can observe a broad
spectrum of an examinee's appreciation of and consideration for tissues,
technical knowledge, and clinical competence. With other so-called permanent
restorative procedures, at least two clinical appointments are required for the
one taking the test to cover the same ground. Consequently, most of our State
Boards require a direct gold restoration as part of the clinical examination.
This makes life difficult for candidates if their alma mater did not teach the
procedure with enthusiasm or competence. It would be so much better if
students were taught the use of foil as a prime restorative procedure, which it
is, rather than as an unpalatable discipline. Then it would be just one of the
familiar facets of their operative repertoire instead of a strange and
frightening testing device.
Interestingly enough, when gold foil is used to control
defective grooves or pits in primary teeth, young patients are unusually
enthusiastic. They display the new acquisition to their friends and schoolmates
with delight and pride, and are great boosters for continued preventive dental
service.
Specific Indications
for Gold Foil
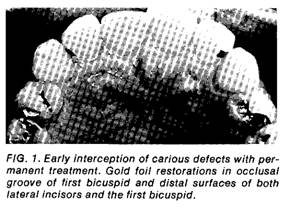
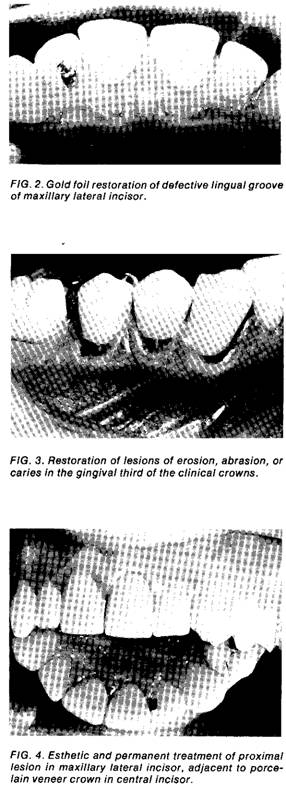
Gold foil, or one of the other direct golds,
is without peer in meeting the requirements of permanent, conservative, esthetic
restorations in a number of areas exhibiting incipient lesions (Figs. 2, 3,
4). Principal indications for use include defective pits and fissures, erosion,
abrasion, or caries in the gingival third of clinical crowns, small proximal
lesions in anterior teeth—maxillary and mandibular—and
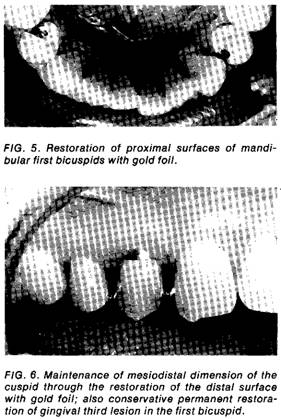
in first bicuspids (Fig. 5). One of the most rewarding uses for foil is to
restore the distal surface of cuspids and thus
preserve the mesiodistal dimension of the arch (Fig.
6). A highly useful indication and an easy operation is the
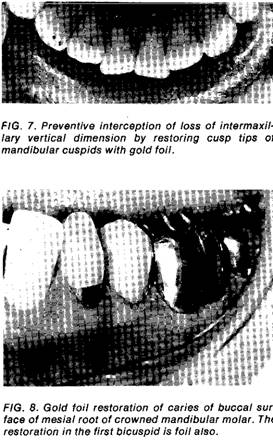
restoration of cusp tips exhibiting
wear through the enamel and cupping of the dentin (Fig. 7). Another excellent
use for direct golds is in extending the margin of an
existing cast restoration. For example, a complete cast crown may be quite
satisfactory, but recession of the gingiva has
exposed a portion of the gingival margin and caries is beginning there. Gold
foil will extend the service of the cast crown conservatively and esthetically
(Fig. 8). If wear by an opposing tooth creates a hole in a cast crown or inlay,
the entire restoration need not be replaced—the area of failure may be restored
with a small repair of direct gold.
On the other hand, direct gold restorations can be
disastrous if there is poor case selection, or if the operating technique in
cavity preparation, material manipulation, or finishing procedure is improper
or inadequate. Examples of improper case selection would be lesions that are
too large, too conspicuous, or too inaccessible, or where the patient's attitude,
general or oral health are contraindications. It must
be recognized that these materials do require more knowledge and expertise
from the operator than can be gained from a "once over lightly"
exposure to the technique. It is not enough to read about it in a book, watch
one film or one clinical demonstration. As with any worthwhile skill, practice
and a real desire and effort to do well are essential. Just because a
restoration is direct gold, the tooth has not necessarily received a superior
service. A poor or mediocre gold foil is perhaps one of the worst restorations
our patients can receive.
Technics
If we are going to offer this refined, preventive
restorative service to our patients, there are some definite requisites. The
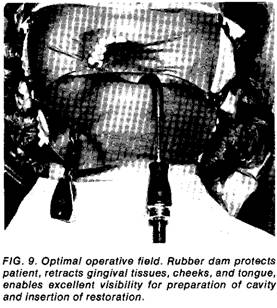
first essential is a proper field, one that is clean and dry (Fig. 9). A simple
dam application, one that is effective and comfortable, that improves rather
than impairs visibility and accessibility, provides the best means available.
At present, many more practitioners use the rubber dam than was the case a few
years ago. While a dry field is obtainable with some of the current holding
devices, operators who work with direct gold freely tend to favor a holding
device
which will keep the edges of the
dam out of the way and which will retract and support the lips and cheeks. Such
a holder also permits use of a comfortable absorbent face mask between the face
and the dam and keeps the patient more comfortable.
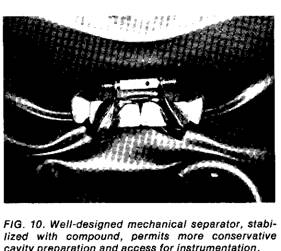
In Class V’s, the field attained with the rubber dam needs
to be supplemented by a suitable retractor, and in many Class III’s by a suitable separator (Fig. 10). The technic of applying and stabilizing these instruments needs
to be performed carefully and well, with
the welfare of the teeth and the
supporting tissues in mind.
Another requirement is a set of good cutting instruments,
hand and rotary, in top condition. As you are aware, we are faced with a
problem of quality control of instruments and supplies due to the current
increase of manufacturers that are not dentally oriented. To perform
restorative procedures expeditiously and well, instruments must have sound
specifications; then we must insist on them being made to those
specifications. A vigilant eye is essential or we will find it more and more
difficult to perform our work properly.
Next, there must be a good cavity preparation that
satisfies the requirements laid down so long ago by G. V. Black. There is
justifiable interest at present in minimal display of metal in restorations, so
preparations are increasingly conservative in outline. Care must be taken,
however, not to carry esthetics to such an extreme as to sacrifice extension
for prevention of recurrence of caries, or adequate convenience for insertion
of gold.
As to the gold used, several forms are now available: foil
in pellet, rope, sheet, or laminated form; mat; powdered gold; alloyed filling
gold; or combinations of these. Each requires a specific technic
if optimum results are to be achieved. In recent years fine research has been
done with the material in its various forms. The reports of Hollenback,
Hodson, Baum, Welk, G.
Smith, Zhonga, Cantwell, and their co-workers, and
others are well worth your attention.
Next, suitable means of preparing and compacting or
condensing the gold are essential. Aside from a means of annealing or purifying
the gold and conveying it to the preparation, these range from hand
condensers, usually supplemented by a mallet, to one of the mechanical
devices—spring, pneumatic, or electronic. Each has its advocates. One must be
aware, too, of the governing principles of compacting gold, the part of the
procedure which is perhaps the most demanding. The operator must understand
proper control of the amount and direction of the compacting force. Even nib
size and serration are important factors.
Proper finishing is particularly important. Improper
procedures will damage the dental and supporting tissues. Careless trimming
with files or knives, excessive use of abrasives, or inadequate coolant can
spell doom for a gold restoration or its host tooth. Extreme care and
meticulous technique are essential to avoid marring tooth surfaces, or bruising
and lacerating surrounding soft tissues. Abuse of tissue is inexcusable.
Correct procedures leave the tooth and supporting tissues in excellent condition,
and the patient and operator should be able to anticipate with confidence a
lifetime of service from such a restoration.
If an individual wishes to increase his competency with
these materials, a few suggestions are offered. One should read some of the
fine papers and monographs on the subject. The forerunner of this new journal,
the Journal of the American Academy of Gold Foil Operators, has published many
excellent articles in the various phases of foil technique. Some of the most
outstanding papers can be found in earlier periodicals in the better dental
libraries. The particular technique and material of greatest interest will
dictate the direction of the individual's search into the literature.
How To Gain Competence
After reading, the next step is to practice the procedure on
the laboratory bench. The chairside assistant should
work with the operator on the technique project so the essentials of team
effort are acquired before going to the patient. Next, one should enroll in a
continuing education course in the use of direct golds.
Finally, if geographic conditions permit, the finest possible avenue to
confidence in the new skill is to affiliate with an active, operating study
club. The regular practice, under supervision, will improve operative
competency in all phases of clinical dentistry as well as in the ability to
utilize the direct golds effectively.
In conclusion, I urge you to retain this means of therapy in
your active repertoire, for there is a definite place for foil in restorative
dental practice today. Our techniques must be current, conservative, and
executed to the best of our ability. Then we may use the direct golds more often, more confidently, and more competently,
wherever indicated.
This Article was scanned and edited By Dr. John R. Sechena