to the wishes of the patient and refrain from the use of the material which he deems best.
Unfortunately, we do not have available any material for the making of permanent restorations which can be regarded as ideal. If such material were obtainable, it should possess the following characteristics
t. It should be perfectly adaptable to all parts of the cavity.
2. It should not be affected by the fluids of the mouth.
3. It should possess sufficient crushing resistance and edge strength.
4. Its resistance to attrition should correspond to that of the enamel.
5. Its color should harmonize with that of the enamel.
6. It should be a non-conductor of thermal impressions.
7. It should be so constituted that it would take and retain a satisfactory surface finish.
8. Its volume changes should correspond to those of the hard tissues of the teeth.
g. It should be easily tolerated by the hard tissues of the teeth and by the soft tissues of the mouth.
10. Its manipulation should be a comparatively simple procedure.
11. Its cost should not be prohibitive. Considering these properties collec
tively, it can be seen that we do not now have any material which can be regarded as completely satisfactory for all types of restorations. We do, however, have materials which lend themselves to the restoration of certain parts of the oral cavity which can be regarded as rather satisfactory for the particular types of restoration for which they are primarily intended.
Let us consider the characteristics of gold foil in relation to those of the ideal restorative material, in order to gain a better understanding of gold foil, an excellent material in many permanent restorations.
Gold is not affected by the fluids of the mouth. There is absolutely no tend
ency toward dissolution of this material by the saliva or any other fluid that is taken into the mouth. This property is necessary to all materials, since it is one of the principal factors in the permanency of a restoration.
Gold takes and retains a satisfactory surface finish, an essential to the maintenance of oral cleanliness and the prevention of recurrence of decay.
No unfavorable volume changes occur after gold foil restorations are completed. Neither shrinkage nor expansion to any appreciable degree can be tolerated in any restorative material.
Gold foil possesses the most desirable property of being perfectly adaptable in all parts of the cavity. This, together
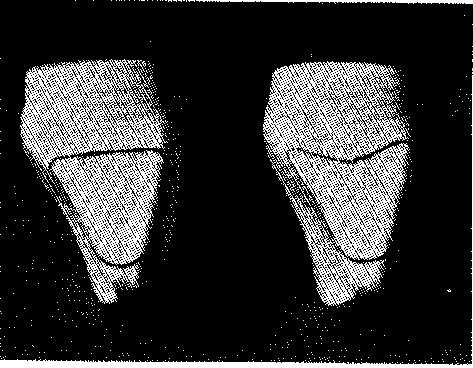
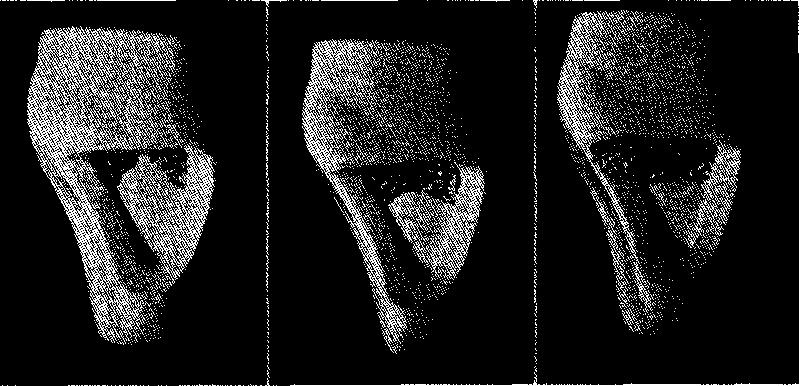
Fig. 1.-Outline forms.
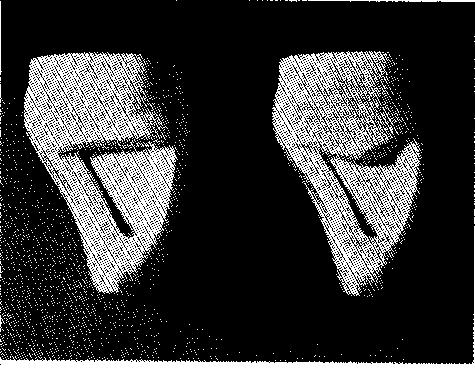
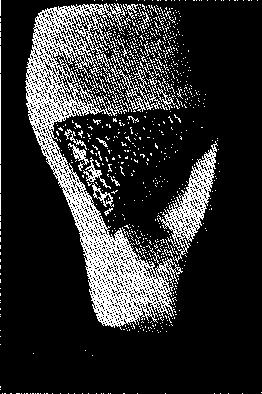
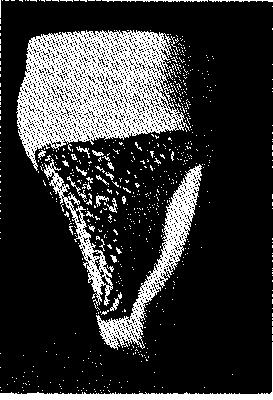
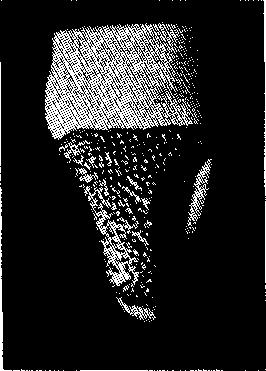
Fig. 2.-Resistance and retention forms.